


 (ii) (b) rule 3A and various insurance companies and TPA\"s. >")
Proximal Femoral Osteotomy- Avascular necrosis of head of femur
Usually seen in younger age groups. The best choice is to salvage the natural hip joint which is definitely better than joint replacement in this age group. Proximal femoral osteotomy is currently commonly used for adults in the treatment of hip fracture nonunions and malunions and in cases of congenital and acquired hip deformities.
The goal of the femoral osteotomy procedure is to alter the contact point across the articular cartilage during weight bearing. When arthritic change occurs without deformity, then a valgus-extension osteotomy moves the contact point of weight bearing forces to a new location on the femoral head, alleviating the pressure across the degenerated area of articular cartilage.
Problem
In young patients with symptomatic hip disease, total joint arthroplasty has traditionally been a suboptimal solution. Problems with accelerated bearing wear and premature implant loosening leading to early revision surgery are well documented in this patient population. Intertrochanteric osteotomy has some use in providing temporary relief of pain in this challenging group of patients. While newer bearing materials with improved wear properties may improve the longevity of total joints in young patients, data to support this position are yet lacking.
Patients with deformity of the proximal femur typically develop arthritis over time because of abnormal joint wear from malalignment. Deformities typically include a varus or valgus neck-shaft angle, rotational malalignments, and leg-length discrepancy in any combination. These deformities can be acquired, as in the case of proximal femur fracture malunions and nonunions, or developmental, as in the cases of fibrous dysplasia, coxa vara, and developmental dysplasia.
Regardless of the etiology, these patients with femoral deformity are at an increased risk for the development of pain and arthritis in the affected hip. Once arthritis has begun, the problem is further aggravated by the mechanical malalignment from the femoral deformity. Standard hip replacement techniques and prostheses are usually unsuitable for deformed proximal femora, thus increasing the complexity of the procedure, surgical risks, and possibly the longevity of the reconstructed joint.
The benefits of early proximal femoral osteotomy to correct the deformity are two-fold. One, in the deformed hip prior to the onset of arthritic changes, the realignment often reduces symptoms, prevents further joint degeneration. In the deformed hip with arthritic changes, restoration of normal alignment can often decreases pain and improves function. Moreover, if the relief of symptoms is incomplete and the patient later requires hip replacement surgery, then the arthroplasty procedure is simplified by restoration of the anatomy
Proximal femoral osteotomy is commonly used in the treatment of nonunions of hip fractures. Both femoral neck and intertrochanteric fracture nonunions respond positively to valgus-producing realignment osteotomies. Malunions of hip fractures, including intertrochanteric type and unreduced slipped capital femoral epiphysis (SCFE), are other common indications for osteotomy. Infrequently, proximal femoral osteotomy is performed in adults for the treatment of hip arthritis and osteonecrosis
.
Indications
The bases for performing a proximal femoral osteotomy can vary. In the presence of deformity, the goal is to correct the deformity and in so doing, realign the hip and lower extremity. This may include frontal, sagittal, and rotational corrections and perhaps even lengthening through the osteotomy. Indications for proximal femoral osteotomy in adults include the following:
- Nonunion of a femoral neck fracture
- Nonunion or malunion of an intertrochanteric hip fracture deformity
- Rotational deformities, as in the case of severe femoral anteversion, SCFE, and developmental dysplasia of the hip
- Frontal plane (varus/valgus) deformities, as in the case of congenital coxa vara, varus fracture malunion, and shepherd's crook deformity from fibrous dysplasia
- Sagittal deformities, including flexion and extension deformity, either bony as in fracture malunion or nonbony, as in hip flexion contracture of achondroplasia
- Significant shortening or bone loss of the distal femur requiring a proximal lengthening
- Combinations of the above indications, as in intertrochanteric fracture malunion with varus, external rotation, and shortening deformity
- Simultaneous femoral osteotomy and total hip arthroplasty
- Hip osteoarthritis or osteonecrosis in the young, active patient Contraindications for femoral osteotomy include:
- The presence of infection may preclude the use of internal fixation; however, external fixation may be a viable option in such cases.
- Limitations of hip motion can make realignment unsuccessful without soft tissue releases or compensation through the osteotomy.
- Advanced osteoarthritis or osteonecrosis is a relative contraindication.
- Inflammatory arthritis can also be a contraindication
X-ray before surgery

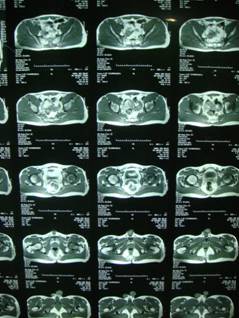
CT-Scan before Surgery
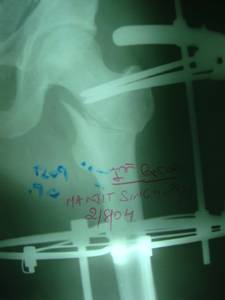
X-ray during treatment


<b>After 4 years of surgery</b>



This young man -29yrs old was suffering from billlateral avascular macrosis of hip joint(femoral head).Left was worst than Right We have done a Proximal femoral osteotomy with ilizarov for left hip and multiple drill holes on the right hip.These are the X-rays before surgery, during treatment and clinical outcome after more than 4 years. There is a very large series of similar cases .