


 (ii) (b) rule 3A and various insurance companies and TPA\"s. >")
RADIUS LENGTHENING
Introduction
The forearm consists of two bones (radius and ulna) and six joints (elbow: radio-capitalar and ulno-humeral; wrist: radio-carpal and ulno-triquetral; radio-ulnar: proximal and distal). Unlike the relationship between the tibia and fibula in the lower extremity the radius and ulna move functionally relative to each other to produce the movement of supination and pronation . Relative to the elbow they move together (flexion and extension). Although most wrist motion and stability comes from the articulation between the radius and the carpus, the ulna provides support for the ulnar side and prevents excessive ulnar deviation of the hand. The relationship between the radius and the ulna is therefore one of the most functional relationships between any two bones.
Exostosis formation of either bone can easily interfere in the function of the elbow, wrist or forearm rotation. Since osteochondromas form from the growth plates they are usually found at the ends of the bones but migrate towards the shaft of the bone with growth. .
|
|
|
|


Radial Osteochondromas: osteochondromas from the radius can be divided into those that protrude towards the ulna and those that don’t. The latter don’t impede supination-pronation motion, while the former do. .
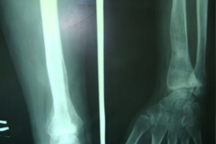
Distal radius deformity: the distal radius has a normal inclination towards the ulna of 23. In MHE the slower growing ulna may tether the distal radius on the ulnar side leading to increased distal radial tilt. This increased tilt appears as ulnar deviation of the hand. With time the carpus will subluxe ulnarly and proximally. .
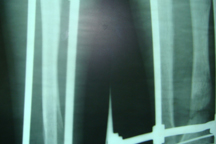
Proximal radius deformity: the ulnar tether also exerts a dislocating force on the radio-capitellar joint. As the radial head subluxes it comes to rest against the lateral condyle of the humerus. To adapt to this chronic position the radial neck may grow into valgus. With time, the radial head may completely dislocate and protrude posteriorly. .
Length discrepancy: The entire forearm is shorter than the other side. The shortening is predominantly in the ulna. Some shortening is also present in the radius. .
Clinical signs and symptoms: Patients are limited in their forearm rotation range of motion. The wrist is usually ulnarly deviated. There may be a prominence or bump if the radial head is subluxed or dislocated. This may be tender to being bumped. Elbow flexion and extension is usually not affeceted. A flexion deformity of the elbow may be present. .
Lengthening Reconstruction Surgery (LRS): LRS refers to distraction surgery using external fixation to lengthen and correct deformities of the forearm. The problem in MHE ranges from simple to complex.
Simple cases: In simple cases, the primary deformity is relative shortening of the ulna. The radial tilt is minimal and does not need to be addressed. There is no subluxation/dislocation of the radial head. The problem is therefore just shortening of the ulna. If this is left untreated the secondary deformities of the radius will develop. The treatment is to perform an isolated lengthening of the ulna.
Complex cases: In more complex cases the surgical plan includes correction of the distal radial deformity and or radial head dislocation. A circular external fixator is used. Proximally both the radius and ulna are fixed. The ulnar osteotomy is made proximally and the radial osteotomy is made distally. This type of frame simultaneously corrects shortening of the ulna and tilt of the distal radius. If the radial head is dislocated then the treatment is staged. The first step is to lengthen the ulna with a pin connecting the radius and ulna distally. This transports the radius distally and reduces the radial head. If the radial head does not reduce spontaneously then at a second stage surgery the radio-capitellar joint is opened and the radial head reduced at surgery and is held with an olive wire. If there is both distal radial tilt and dislocation of the radial head then the radial head is reduced first and then at a second stage the wire pulling the radius and ulna distally is removed and the distal radius osteotomized for deformity correction and lengthening